
Ghana is preparing for a major shift in primary healthcare that could reshape outcomes for millions. The Ghana Health Service has announced an ambitious push to ensure that every single health worker — from ward cleaners to senior consultants — receives training in basic life support and emergency response as the nation rolls out a Free Primary Healthcare policy. This initiative is positioned as a cornerstone of Ghana’s drive toward Universal Health Coverage by 2030 and is designed to reduce preventable deaths, strengthen pre-hospital care, and make frontline facilities more resilient and responsive.
The policy’s timing and scope matter. Set to begin in early March 2026, the Free Primary Healthcare program promises free access to promotive, preventive, and basic curative services, with a strong emphasis on early detection and management of non-communicable diseases such as hypertension, diabetes, and certain cancers. To make that promise real at the community level, facility leaders must change how they think about long-term service delivery, embedding the program into everyday practice rather than treating it as a short-term project.
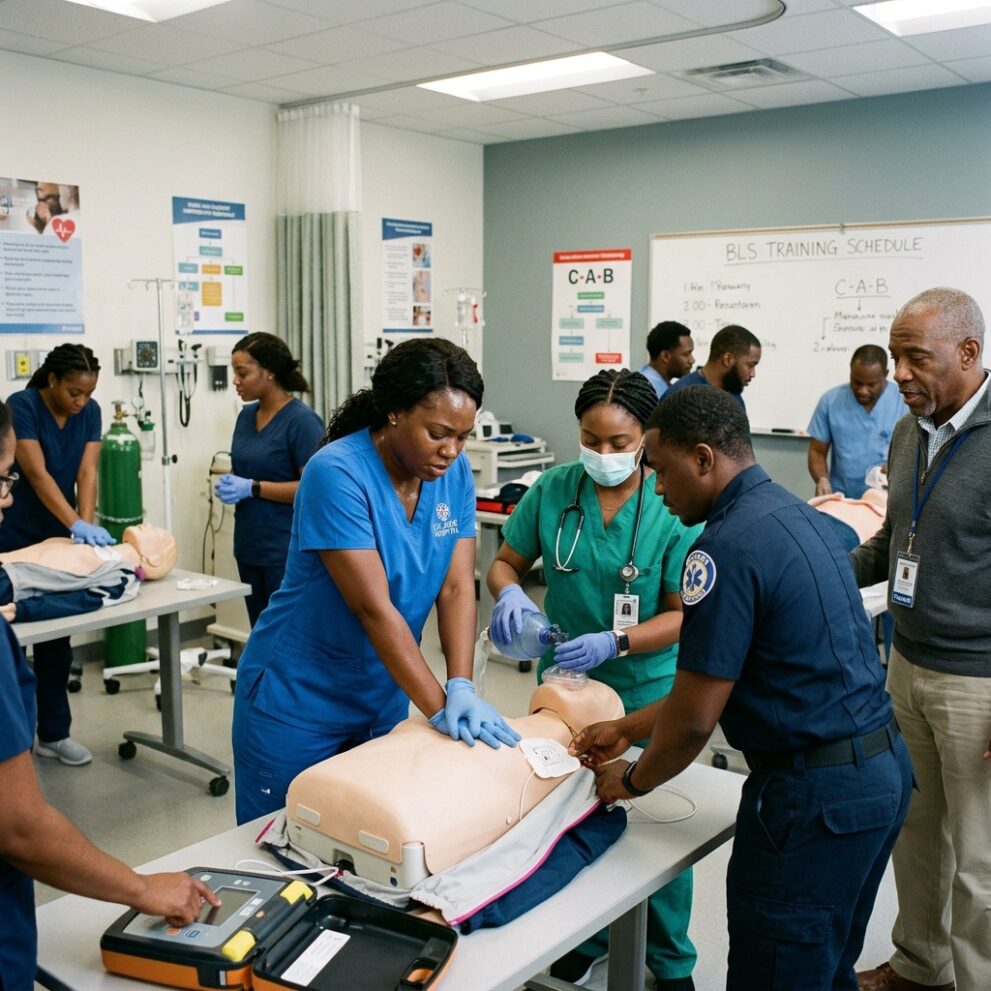
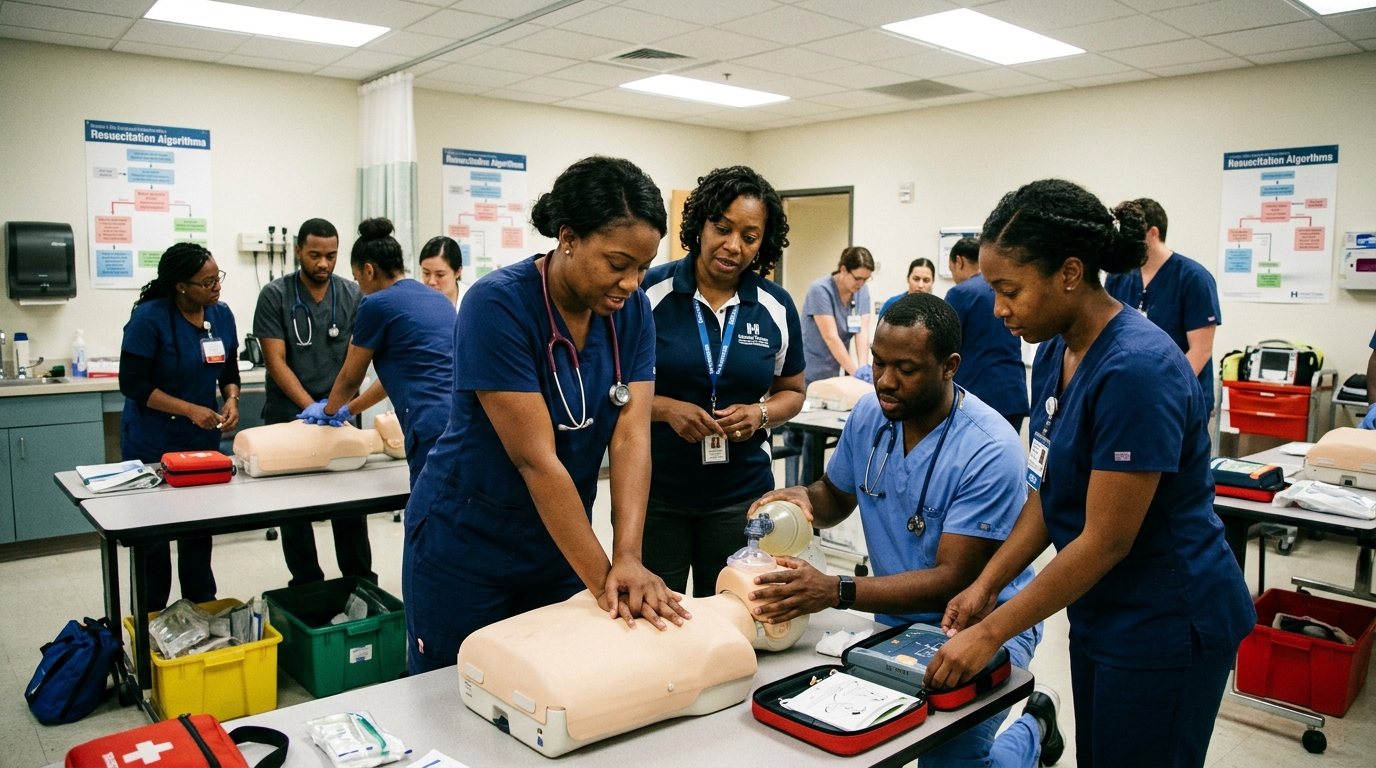
Training every health worker in basic life support is a bold, systems-level intervention. The Director-General of the Ghana Health Service, Dr Samuel Kaba Akoriyea, explained the logic plainly: emergencies require coordinated action at both the pre-hospital and hospital stages, and the first responders are often the people already on site. “When it comes to emergencies, normally we need to look at the pre-hospital stage and then the hospital stage. Everybody needs to be trained in basic life support,” he said, stressing that the plan covers the entire workforce. This single strategic move — universal basic life support training — can dramatically shorten the time to critical interventions and improve survival rates for cardiac arrest, severe trauma, and other acute conditions.
Beyond training, the policy includes concrete investments to upgrade ambulance services and strengthen referral systems so that critical cases can be stabilized and transferred safely. Strengthening referral pathways means equipping frontline facilities to handle emergencies before transfer, improving communication between levels of care, and ensuring ambulances and transport logistics are reliable. These operational upgrades are essential because training alone cannot save lives if patients cannot reach higher-level care when needed.
The financial commitment behind the plan signals serious intent. The 2026 national budget allocated GH¢34 billion to the health sector, representing more than 11% of total government expenditure, and the Ghana Medical Trust Fund — known as MahamaCares — received GH¢2.3 billion to support patients with non-communicable diseases. These allocations create fiscal space for training programs, ambulance upgrades, and the supply chains needed to sustain improved emergency response across regions.
Why this matters for public health and for search audiences worldwide: preventable deaths from late presentation of disease are a global challenge, and Ghana’s approach combines workforce capacity building with system-level investments. By training non-clinical staff in basic life support, the country expands its first-response capacity exponentially. By pairing training with better ambulances and referral systems, Ghana addresses both the human and logistical barriers that currently allow treatable conditions to become fatal. This dual strategy is the kind of integrated health systems thinking that public health experts recommend for low- and middle-income countries aiming to accelerate progress toward Universal Health Coverage.
For health leaders, the operational implications are clear and immediate. Facilities will need standardized training curricula, regular refresher courses, and competency assessments to ensure skills are retained. Supply chains must deliver essential emergency equipment — automated external defibrillators where feasible, oxygen delivery systems, airway management tools, and basic resuscitation kits — to the places where trained staff work. Data systems must capture emergency response metrics so that policymakers can measure impact: time to first intervention, stabilization rates, referral times, and survival outcomes. These measurable indicators will be crucial to demonstrate that the policy is saving lives and to guide iterative improvements.
Community trust and awareness are equally important. Free services will only be used effectively if communities understand what is available and when to seek care. Public information campaigns that explain the scope of free primary healthcare, the signs of common emergencies, and the role of trained frontline workers can increase early presentation and reduce delays. When citizens know that even non-clinical staff can provide immediate life-saving measures, they are more likely to seek help quickly, which in turn improves outcomes.
There are challenges to anticipate. Scaling training to every health worker requires trainers, time, and funding; maintaining quality across hundreds of facilities is complex; and rural areas with limited infrastructure will need tailored solutions for ambulance coverage and referral logistics. However, the policy’s comprehensive funding and the explicit focus on embedding the program into routine health delivery — rather than treating it as a temporary campaign — increase the odds of sustainable success. Strategic partnerships with training institutions, NGOs, and international health agencies can accelerate capacity building and provide technical support where needed.
This initiative also creates opportunities for innovation. Mobile training units, blended learning platforms that combine short in-person skills sessions with digital refreshers, and community first-responder networks can extend the reach of formal training. Telemedicine and real-time communication tools can support frontline staff during emergencies, enabling remote guidance from specialists while patients are stabilized and prepared for transfer. These innovations can make the training more effective and the referral system more resilient.
To summarize the core takeaways in plain terms: Ghana’s Free Primary Healthcare rollout is more than a policy announcement; it is a systems transformation that pairs universal access with a workforce-first strategy to save lives. Training every health worker in basic life support, upgrading ambulances, and strengthening referral systems are complementary moves that, together, can reduce deaths from emergencies and late-stage disease. The government’s budgetary commitments provide the financial backbone, but success will depend on implementation fidelity, community engagement, and continuous measurement. “The mindset of facility leaders must shift fundamentally,” the Director-General warned, and that cultural shift — from short-term project thinking to permanent integration — will determine whether the policy achieves its life-saving potential.
This policy moment is an invitation to reimagine primary care as the first line of life-saving defense rather than merely a gateway to higher-level services. If Ghana succeeds, the model will offer lessons for other countries pursuing Universal Health Coverage: invest in people, pair training with logistics, and make emergency readiness a routine part of primary care. The result could be a measurable decline in preventable deaths and a stronger, more equitable health system for all Ghanaians.
Source: GHS Boss Wants Every Health Worker Trained in Life-Saving Skills | NewsGhana

